

Sommario


Translated by Concetta Violante
The subject I am on the point of discussing presents a very wide interdisciplinary range and consequently my approach will necessarily be partial, but I will not fail to use some direct clinical experiences and I will try to shelter from that speculative nature against which Freud always feared to have to protect his students and the development of psychoanalysis much more than his work (always obstinately linked with clinical instruction and research).
A relation between psychoanalysis and neurosciences is not actually absurd when one considers the solid neurological grounding of psychoanalysis and recognizes its following consistency.
In a recent article by Solms and Saling, published in Italy at the end of the year 2004, the authors discuss the question of the importance of “The interpretation of aphasias” (Freud, 1891), for the following development of Freud’s studies: besides remembering that the author never dissociated himself from this work of his (differently from the Project of a Psychology), for the first time some concepts, which will constitute focal points for psychoanalysis, are used here in their original neurological sense: I am referring to regression, over- determination (Stengel 1953-54), projection, cathexis, presentation and fixation to a traumatic event (“the patient keeps the proposition of the time of his trauma”).
In that essay, following Jackson’s theories, Freud refused his time’s tendency to locate the different pathological expressions in specific zones and supported his theses right with a disorder characterized by an undisputed neuroanatomic location: it was the clinical practice, careful and discerning, and listening, used as a conditio sine qua non by the psychoanalytic method, which allowed to go beyond a neuroanatomic approach and look for a neurophysiological one.
Nowadays this modality is widely shared in clinical neurology where it is ment that the complex mental phenomena cannot be located in distinct cortical or subcortical zones but an appropriate psychological analysis is required.
The approach to dream as the satisfaction of a wish, too, a result of a regression, found its origin in “The interpretation of aphasias” and came out then in the work “The interpretation of dreams”.
The interpretation of aphasias is then considered by Solms and Saling to be the missing link between the neurological period and Freud’s psychological one.
Only after his death neurophysiology began developing what today is called “dynamic neuropsychology” with Luria’s studies, although this development has never been considered by psychoanalysts, which Kandel, too, regrets; let’s remember that Kandel won the Nobel prize for medicine and neurosciences with his studies on memory. In an article of his, written in 1999, he says that “although biology has made progress in the last 50 years, there isn’t yet a satisfactory biological model for the grasp of complex mental processes” and maintains that psychoanalysis is the instrument that could “re-energize itself” by combining with the knowledge of neurosciences.
SLEEP
Neurophysiology made clear several decades ago that sleep is a differentiated activity and that the mammals on our planet (but a large number of birds, too) spend their lives between waking, REM sleep and NREM sleep.
The analogies between waking and REM sleep are surprising:
– the “desynchronized” rhythm of waking is resumed (unlike the NREM synchronous rhythm).
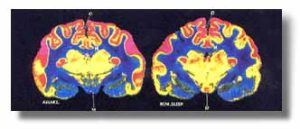
– metabolism rises, as PET images show: these point out a central metabolic rate of glucose utilization even higher during REM sleep than during waking.
The REM and NREM sleep distribution generators are not known but some elements indicate that the former depends on the latter:
– for instance, it takes 90-120 minutes’ NREM sleep before a REM sleep phase takes place.
– during NREM sleep the glucose and oxygen consumption of the cerebral cortex goes down but the energy supplies are stored up as glycogen in the glia. On the contrary during REM sleep metabolism goes up.
– the flow medium speed in the cerebral middle artery goes down during NREM sleep and rises during REM sleep.
– The 02 consumption is reduced by
25% during NREM sleep, whereas during REM sleep it is the same as during waking From the neuroanatomy point of view one can identify the zones that bring about most of the processes connected with waking, REM and NREM sleep:
– waking generators are diffusely placed in the BRAIN AXIS (Reticular Activating System)
– NREM sleep generators are placed in the BULB and in the Basal PROENCEPHALUS
– REM sleep generators are placed in the BRIDGE
Yet the components of waking, REM and NREM sleep are modulated by very complex phenomena that involve various levels of the neuraxis and different neurotransmitters.
But no part is accountable for a specific kind of sleeping as studies on animals clearly reveal:
Actually each kind of sleep, if inhibited by a non- lethal lesion, tends to occur again.This indicates that different parts of the CNS can generate sleep. A possible conclusion of these considerations is that
– SLEEP IS A BASIC PROPERTY OF NUMEROUS GROUPS OF NEURONS;
– SLEEP IS PRESUMABLY REGULATED BY LOCAL FACTORS RATHER THAN A PHENOMENON THAT NEEDS THE WHOLE ENCEPHALON OR SPECIFIC ZONES.
It seems to me that this concept, once again dynamic-functional, besides being consistent with what Freud observed in aphasias, refers back to Jouvet’s concept of SEISMIC SLEEP, taken up again by Fanti (to demonstrate his theory of the Neutral Dynamism of Vacuum).
SEISMIC SLEEP
In the first ‘70s, starting from the hectographic series of sleep in premature babies, various neurophysiologists identified the absolute majority of REM sleep and another kind of tracing accompanied with a body motility marked with shocks of various width, clonic contractions and an EEG tracing different from REM-NREM and defined “undifferentiated”. After 7 months’ intrauterine life a period of REM phases shows up progressively and persists until birth and for the first weeks. “Until the end of neurogenesis and the beginning of homoeothermy”, says Jouvet.
Jouvet maintains that there is an inverse ratio between neurogenesis and REM sleep not only in ontogenesis but also in phylogenesis:
1) there isn’t paradoxical sleep in cold-blooded animals (heterothermics). Neuroblasts duplicate themselves as every cell and guarantee genetic programming.
2) birds are the first on the zoological scale to show REM sleep, but much less than mammalia.
3) in mammals seismic sleep disappears with neurogenesis
4) on the zoological scale the transformation of the heterothermic state into homoeothermy is characterized by the end of neurogenesis and by changes that take place in the brain (appearance of archistriato in birds and appearance of neocortex in mammals) and at general level (significant increase in mitochondria and in energy processes, with the transformation of bradymetabolism into tachymetabolism).
But can the appearance of paradoxical sleep (REM) in zoogenesis as in fetal life ensure an iterative programming in the species in which neurogenesis ceases at the end of ontogenesis? Studying the quick eye movements of monozygotic and dizygotic twins Jouvet answers in the affirmative.
Today valid arguments explain that the periodic and regular stimulation of the neural system is necessary to preserve the CNS function and that REM sleep is necessary to the prenatal development and the post-natal keeping of the brain function.
DREAM
After the first neurophysiological discoveries occurred about 50 years ago, after the discovery of REM sleep (a synchronous bioelectric activity) and NREM sleep (a desynchronized bioelectric activity) and after the conceptualization of Seismic Sleep (an undifferentiated bioelectric activity), what are the relations between these activities and the sum of memories and emotions we have when we wake up and which condition our days, moods, choices and health?
To give a short example of how a dream can influence waking life I will use a dream of a little girl, since childrens’, psychotics’ and old peoples’ manifest content is more similar to the latent one; I will therefore avoid going into associations and interpretations.
In her night theatre the little girl, who is in her latency period, cuts out a picture from a periodical. It is a feline monster that becomes animated and jumps into the house. It starts wandering about the rooms, which are dreamt as they were before the little girl’s grandfather’s death and the birth of a brother of hers. While everybody is running away, the monster gets to her mother, who is undressing in her room, and attacks her but she manages to defend herself and tame it.
When the little girl wakes up she is uneasy and the pictures of her dream still fill her mind; she shows her mother a bad mark and the woman gets angry like a wild animal: now she will have to go to the school to speak to the teacher. The little girl bears the reproach but gets deeply angry because of what, she thinks, is an injustice and the uneasiness caused by her dream ends.The dream has worked well: it has allowed a displacement from a position of self- incrimination (in her dream the little girl unleashes a beast in the house; after waking up it is she who shows the mark and so causes her mother’s reproach-punishment) to a position of anger.
Actually that reproach is unjust because she is a very clever pupil and has been given a bad mark because of banal disciplinary reasons, so she can get angry at her mother: therefore everything is all right until a new rise of tension.
We have thought for a long time that dream was a prerogative of a REM phase: it is certain that vivid and evocative dreams occur during REM sleep.
Thanks to the studies of Solms (1995,1997) and Kaplan-Solms (2000) on dream processes, we know today that REM sleep and the dream activity belong to different anatomic structures and that the fundamental mechanisms of dreaming are not regulated by the deep brain structures of the encephalic trunk, which, on the contrary, regulate the physiologic mechanisms of REM sleep, but by zones of the front brain and particularly of the lower part of the parietal lobes and of the middle-basal part of the frontal lobes.
The anatomic structures of the front brain related to the phenomenon of dream construction are those taken up with the functions of emotions and memory (the limbic system, including the limbic components of the front and temporal zones, that is to say the parietal-temporal- occipital junction, and the system of the visual zones). This means that the control of REM sleep is a prerogative of structures that are phylogenetically older, whereas the dream activity takes place in brain zones of a more recent phylogenetic development.Then we have known
that there is a certain dream activity in NREM phases, too:
The presence of a mental activity similar to the one registered during a REM phase was proved to be also in NREM phases and during falling asleep by Bosinelli (1982), Bosinelli & Cicogna (1991) and Foulkes (1962, 1985).
This mental activity consists of dreams that are less remembered or sometimes leave the memory of a thought rather than of actions and complex situations as the ones dreamt during REM sleep. According to these authors the elaborating modes in the two types of sleep (REM and NREM) are completely similar, which suggests a single dream activity production system, active during each phase of sleep even though in a different measure.
Micropsychoanalysis has always been interested in these data deriving from neurosciences. The attention paid to the repetition of phylogenetic traumatisms faces, for instance, the concept of genetic repetitive programming done by REM sleep and allows to examine the different phenomena related to dream with an integrated perspective.Besides, this is required by psychoanalysts’
growing care in clinically severe situations and against a rise in the number of involutional pathologies because of the population’s ageing, the growth of dietary disorders and an increase in the diseases related to a chronic excessive use of toxic substances.In a psychotic suffering from an acute phase it can be difficult to distinguish reality from dream; or we are struck by the hiatus between the falling apart of thought and what appears as the normality of dreams: their manifest content is not unlike the so-called “healthy” population’s or, to be more precise, children’s.
As it is known, in bipolar disorders,sleep disturbances (insomnia or hypersomnia) are one of the symptoms which the diagnostic criteria of DSMIV are founded on.
disturbances:
– patients may have no difficulties in falling asleep but report a central insomnia with a difficulty in falling asleep again (precocious awakening);
– the moment of awakening in the early morning is statistically the highest-risk time of suicide;
– hypersomnia is rarer than insomnia;
– REM phases grow in hypomanic dysphoria and the decrease in REM sleep is considered essential for a redressing of the affective sphere in bipolar patients in depressive phases;
– these patients also present an increase in glucose metabolism during the first NREM period, which is, as we have seen, the preparatory metabolic phenomenon of REM phases, the accumulation of the energy necessary to the great work of dream.
The data on sleep deprivation show that the total deprivation of sleep (REM & NREM) is fatal to animals in about 3 weeks. The mere deprivation of REM sleep is fatal in 6 weeks. Yet many animals survive and are seemingly normal if one intervenes at the last moment.
Of course it is not possible to perform similar experiments on man.
Nevertheless let’s think of the FAMILY FATAL INSOMNIA, which belongs to prion diseases, which are disorders due to the production of a modified form of the prion protein synthesized by a gene on the short arm of the chromosome 20. This disease, with a course that lasts from 1 to 4 years, causes the complete passing of all the circadian rhythms and of neuroendocrine rhythmicity. The presence of myoclonias and behaviours similar to hallucinatory dreams suggests a disorder of REM sleep behaviour or of a dissociative state.
Even though death due to the family fatal insomnia must be imputed to a more complex totality of factors, the passing of sleep and dream functions is not the last one.
We know that some medicines commonly used to treat bipolar disorders, as the IMAO, TCA and SSRI, cause REM sleep suppression and that this is considered to be one of the therapeutic effects of these medicines.
It is admissible now to examine this partial increase in REM sleep in bipolar disorders after discussing the functions of sleep.
In a 1987 publication, Zangrilli discussed some forms of alcoholism related to precocious psychic trauma and supported by a primary appetition for heat.
Speaking of the case of an abandoned infant, later become an alcoholic, the author maintained that the inexorable repetition compulsion mechanism ordered the search for heat through alcohol and that this search invariably turned then into a loss of heat because of a secondary peripheral vasodilatation.
The whole trauma had occurred when it was impossible to speak of mental organization of experiences: the first neonatal weeks or the last weeks of intrauterine life can be considered to be linked with sense and motion experiences that can be reorganized in mnestic traces only afterwards.
In the REM sleep behaviour disorder patients present a violent tendency to carry out dreams that are potentially dangerous to them or their bedfellows. This behaviour manifests itself during REM sleep and is usually aggressive or exploratory but never appetitive (for food or sex). There is a strong link between distorted dreams and the carrying out of dreams, which indicates a common physiopathology: the patients do not carry out their habitual dreams but the clearly distorted ones, which usually drag into quarrels, assaults and violence.
This description of the REM sleep behaviour disorder is reported in the journal “Continuum”, vol. 1, n. 3, Sept. 1999.
Now let’s see some other relations between REM sleep and aggressiveness.
In his book M. Jouvet makes a remark of great interest for the understanding of REM sleep as a “genetic iterative programmer”: “The more an animal is safe during its sleep….the more the amount of “dream” ( that is to say REM sleep) grows. On the contrary hunted species (herbivores) present only a very small quantity of paradoxical sleep”.
The observations of paleoethnology seem to agree too: in a forthcoming piece of work on Dietary Disorders, Emmanuel Anati points out that vegetarian aborigines were different from carnivorous ones: they were slower and less enterprising.
Therefore we know now that REM sleep not only appears late on the zoological scale but is also greater in carnivores than in herbivores; when it expresses itself in the RSBD, it “shows” its openly aggressive face and grows in bipolar disorders.
I would like to try to discuss this point in the light of the concept of REM sleep iterative programming, of which neurophysiologists speak, and in the light of the functions of homeostasis keeping and onto- phylogenetic trauma reworking by micropsychoanalysts (Fanti & Peluffo).
As for bipolar disorders one of the most delicate problems psychiatrists have to solve is aggressiveness: it should be pursued to shake the subject out of the torpor of depression, or it should be modulated to control the excesses of manic phases, but solutions of true stability cannot always be found in spite of the undisputed advantages of the psychopharmacological records available today.
The tension rise caused by the inhibition (also motor inhibition) of the depressive, who is kept from the usual channels of abreaction and from the restriction to sexuality, is the cause of a risk of suicidal acts. If the same pressure manages to turn into the channelof a manic sortie, it risks being beyond control and causing, in turn, acts that break the homeostatic keeping of the psychophysical unity: that is to say that the subject can injure him/herself and other people.
Dopamine is introduced into this severe and unstable situation.
The dissociation between dream and the various conditions of brain activation from a biomolecular point of view, of which I have already spoken (Solms, 1999), shows that dream occurs when the dopamine circuits of the front brain are activated. These circuits are the common final way that produces dream, besides the various forms of brain activation in sleep (that is REM and NREM; we cannot speak of SEISMIC SLEEP).
As we know,Dopamine is the neuromediator involved in the forms producing psychoses and we also know that historic antipsychotic medicines firstly had a mechanism of action opposing dopamine. The same biomolecular mechanism is involved in the abuse of cocaine and psychostimulants (with well- known hallucinogenic effects).
The discovery that dream occurs when the dopamine ways are activated is a confirmation of so many clinical observations: that dream is after all a hallucinatory modality; that delirium is a dream that storms into waking life in the overbearing manner of the primary process; that delirium is a fragment of a dream not elaborated by the work of dream: one would say that everything is “biochemically true”.
Moreover in bipolar disorders REM sleep increases and therefore a situation similar to the condition of psychoses occurs:
dopamine increases, at least at the level of the dopamine circuits of the front brain.
What does the organism try to do with this dopamine activation in a situation of bipolarity? For one thing a programme of activation at synaptic level is reiterated by dreaming. Then, if we consider what Jouvet maintains, starting from the phylogenetic data the organism tries to repeat the programme. Finally, Freud would say, it tries to lower the tension at least by hallucinating a behaviour of attack. But the affective disorder has a limitation and anchorage in that: inhibition. Actually, a patient of mine, who has known psychotic thought, says: “unfortunately I must retire a little at those moments, otherwise I would be fixed on a look and then those antidepressive thoughts would be back in my head: that spies follow me, that television speaks to me, that I am at the centre. Do you know that I have become aware of their recurring? But when I had them I was well, I felt important! Eh, I was better when I was worse….”.
I think that the patient with an affective disorder tries to get those “antidepressive thoughts” from dream. It is an attempt of treatment. A treatment looked for in the reiteration of the store of behavioural patterns, mostly aggressive and peculiar to our species. But the attempt fails: the repetition makes the patient revive the series of psychic experiences generating anguish, peculiar to his/her ground and inscribed in his/her dreams and then the inexorable mechanism of repetition compulsion takes him/her back to the starting point.
At the beginning of chapter 4, in “The interpretation of dreams”, Freud says: “I shall then interrupt my exposition because I have come to the point where the problem of dream leads to greater problems, which can be solved only by using another kind of material”……”….after putting aside every reference to the work of interpretation, we can become aware of how much our dream psychology is incomplete. ….but from now on, from the moment when we decide to penetrate the psychic processes of dream in a deeper way, every path will lead to darkness……but the psychological hypotheses we reach in the analysis of dream processes, will, to say so, have to stop off until they have found the connection with the results of other researches, which, starting from other points, intend to get to the bottom of the same problem”.
Now I think that today we have these starting points and I am not the only one who thinks so: we have only to work.
Bibliography:
− Baldari L., Omaggio a Freud neurologo, in Scienza e Psicoanalisi, 2000.
− Fanti S., La Micropsicoanalisi, Borla, Roma, 1983.
− Freud S. (1891), L’interpretazione delle Afasie,Sugarco Edizioni, Milano, 1980.
− Freud S. (1895), Progetto di una Psicologia, in “Opere” Vol. 2, Boringhieri, Torino, 1979.
− Freud S. (1900), L’interpretazione dei sogni, in “Opere” Vol. 3, Boringhieri, Torino,1979.
− Jouvet M., Il sonno e il sogno, Guanda, Parma, 1993.
− Jung C.G., Scritti, Boringhieri, Torino,1961, pag. 191
− Kandel E.R., A new intellectual framework for psychiatry. American Journal of Psychiatry, 1998 Apr;155(4):457-69.
− Kandel E.R., Biology and the future of psychoanalysis: a new intellectual framework for psychiatry revisited. American Journal of Psychiatry, 1999 Apr; 156(4):505-24.
− Kavanau J.L., Memory, sleep and the evolution of mechanism of synaptic efficacy maintenance. Neuroscience 1997; 79.7-44.
− LeDoux J., Il Sé sinaptico. Raffaello Cortina, Milano, 2002.
− Marks GA, Shaffety JP, Oksemberg A, et al., A functional role of REM sleep in brain maturation. Behav Brain Res 1995; 69:1-11
− Mura A., Leggendo Kandel – parte II, in Scienza e psicoanalisi, 2004.
− Peluffo N., Aspetti epistemologici dell’attività associativa ed onirica. In Bollettino dell’Istituto Italiano di Micropsicoanalisi n. 29-30 , Tirrenia Stampatori, Torino, 2001.
− Peluffo N., Elaborazioni oniriche dei derivati di fissazioni utero-infantili; in Bollettino dell’Istituto Italiano di Micropsicoanalisi n. 19, Tirrenia Stampatori, Torino, 1995.
− Scalzone F., Zontini G. (a cura di), Tra psiche e cervello, Liguori Editore, Napoli, 2004.
− Zangrilli Q., Traumi intrauterini e alcolomania,in Bollettino dell’Istituto Italiano di Micropsicoanalisi n. 4, Tirrenia Stampatori, Torino, 1987.
© Gioia Marzi
La Dott.ssa Gioia Marzi è nata a Roma il 30 maggio 1952.
Psichiatra e micropsicoanalista, dal 1980 lavora presso il Dipartimento di Salute Mentale di Frosinone e, dal 2005, è responsabile del Servizio per i Disturbi Alimentari e Psicopatologia di Genere. Docente presso il corso di Psicologia e infermieristica in Salute Mentale – Modulo: Psichiatria – Universita’ La Sapienza – Roma. Ha una vasta esperienza di psichiatria forense in materia di violenze e abusi sulle donne e sui minori. Autrice di numerose pubblicazioni scientifiche, collabora con la rivista Scienza e Psicoanalisi curando la rubrica di psichiatria dal 1999.
Esercita a Frosinone e a Roma dal 1985.














{kind=link}