

Sommario

Can we talk about loneliness of the fetus or loneliness experiences related to pregnancy and birth?
As we are a psychoanalist and an ostetrician gynecologist, we have compared our clinical experiences and ended up with the following hypothesis: loneliness experiences date back to some particular moments of intrauterine life. When these experiences occur frequently, they can provoke serious consequences in mother-child interaction after birth and in their life.
More precisely we assume that lack of progressively growing object investment (otherwise called bonding), due to biological or psychological reasons, can provoke implications in psychobiological development of the baby and in his attachment style. Long depressive reactions and detachment to the baby have been registered in the mothers.
Hitherto the prevailing conception in public and scientific circles was that fetal life resembled a state of sedation mediated by high levels of placental progesterone and neuro-inhibitors in the fetus, and that sensory systems and central processing of external stimuli were probably not adequately developed to perceive for example pain (Mellor et al 2007).
With advent of 4D or real time 3D- ultrasound however, straightforward visual transfer of fetal movements to the sonographer’s eye had become possible. The human eye can differentiate single images up to a frame rate of 12Hz. Above this frame rate, serial images are perceived as continuos movement. Presently, peak frame rates of high end ultrasound machines can reach 20Hz, with still acceptable image quality. This enables visualization of even small facial twitches and has opened the door to an abundant variety of fetal behaviors.
The use of 4D ultrasound in all three trimesters has boosted our knowledge about fetal behavior. Old scientific conceptions of prenatal existence have to be discarded in view of 4D ultrasound revelations of fetal life. 4D ultrasound mediated scientific analysis of fetal behavioral patterns contradicts assumptions of continuos fetal sedation during pregnancy. Observation of a multitude of behavioral features of the unborn similar to those of the newborn prove continuity of fetal and neonatal behavior. Beside these new insights in fetal behavior, recent research has made substantial contributions to our knowledge about the developmental timelines of fetal sensory systems: initiated with the somestetic/proprioceptive systems (tactile/thermo-reception) on the face, palms, and soles at around 7 weeks gestational age (GA), progressive brainstem maturation enables the vestibular system at around 15 weeks. The oral/nasal chemoreception starts to function at the same time, the auditory system develops from 20 weeks onwards, followed by the arrangement of the visual system. (J.P. Lecanuet, B. Schaal, 2002).
As a result of all these new findings, the question of fetal awareness was up for discussion. The developing proprioceptive “inner world” of the fetus and his gradual opening up to external sensual stimuli find their representations in the ‘primary awareness’ of the fetal brainstem. Primary awareness can be understood as a compound of pre-comptences for fetal-maternal attachment. The fetal motoric and sensual equipment and it’s successful development within the maternal organism on the one hand, and the harmonic psycho-physic transformation and maturation of the woman into a mother on the other hand, are linked in dialectic inter-independence.
The sensual interface between fetus and mother has many variables: vestibulo-cochleal, chemosensory, auditory, tactile, psycho-vegetative, endocrinological, and bio-rhythmic stimuli are continuously changing the fetal environment. It is postulated that the fetus memorizes such sensual experiences (specifically, the hippocampus, amygdala, anterior and mediodorsal thalamic nuclei, and mamillary nuclei); these structures are already well developed and functioning at full term gestation. There is for instance evidence that the human fetus has the ability to detect and record odour information afforded by the mother through her diet. (3)
Several studies in animals have demonstrated the persistence of intrauterine acquisition of odour preferences untill weaning or adult age. (4)
According to B. Schaaal and other researchers, this raises the possibility that intake of flavor-rich food, drinks, of tobacco, alcohol, or other addictive substances, may have latent and deferred effets on the behavior of the offspring. (5)
The morphological development of the inner ear – Cochlea – is completed at 20 weeks. Auditory evoked potentials in premature born fetuses can be registered from 24 weeks: vibro-acustic stimulation produces a fetal motor response. Exposure to voice, music, and meaningful sounds after 30 weeks enables the configuration of tonotopic columns on the outer surface of the auditory cortex of the temporal lobe, a process called ‘tuning’. The first in-vivo evidence of the fetal hearing was delivered by non-invasive magnetoencephalography (MEG) brain imaging in 1999.(6)
It is known that the fetus recognizes the mother’s voice from prenatal exposure and is able to discriminate between different speech sounds in utero. This may have implications for development of language, for recognition of the mother and father, and development of attachment.(7)
Visual evoked responses were measured in fetuses from 28 week’s gestation onwards. (8)
There is more new evidence that such actions capabilities develop already early intrauterine. Umberto Castiello and coworkers of the research group around Vittorio Gallese at Parma University found that, starting from the 14th week of gestation, twin foetuses plan and execute movements specifically aimed at the co-twin. For the purpose of this study they analyzed the adbominal four dimensional ultrasound video sequences of 10 fetuses each recorded for 20 minutes. The video recordings were then digitized through special software allowing off-line kinematic analysis of hand movements. Their study results lead to the assumption “…as fetal behaviour patterns directly reflect developmental and maturational processes of the fetal central nervous system, it might be advanced that social patterns might represent early markers of the appearance of developmental disorders affecting the social dimension of behavior. (9)
Loneliness in fetal-maternal relation can be caused both by biological and psychological disorders. We consider biological disorder pregnancies in mothers with the apallic syndrome (the so called ‘frosen mother’) and the “fetal akinesia-deformation sequence” and we refer to our recent case. As regards the psychological disorders, we refer to different cases of mothers with narcissistic traits that affect the attachment.
Maternal loneliness
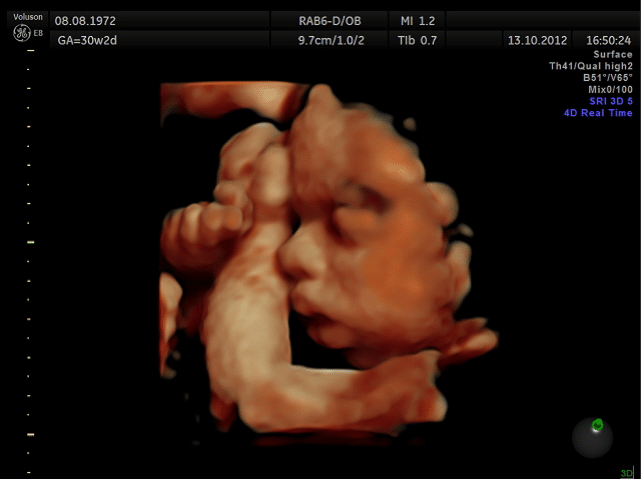
immobile fetus at 31 weeks
We are reporting the case of a 40 year old 2nd gravida, 1 para, with spontaneous pregnancy. This lady had an eventful previous medical and obstetrical history of an uncomplicated first pregnancy, with normal vaginal delivery term. In this pregnancy she had normal pregnancy surveys with normal ultrasound(US) scans at 6 and 8 weeks. Though she changes her obstetrician twice until 26 weeks, she adhered to regular checkups with he obstetrician every 4 weeks. She felt fetal movements first a 18 weeks and emphasized that they were more frequent and vigorous than in her first pregnancy when she started to notice fetal movements only at 21 weeks. At 26 weeks of the reported pregnancy, fetal movements stopped suddenly and almost completely within 24 hours. She went to an emergency unit where she was reassured. At 30w2d she was referred for Doppler scan and fetal biometry. In US normal morphology was detected. Biometry corresponded to 28w1d. Abdominal circumference minus 2,4 SD, cerbellum diameter minus 2,2 SD indicated moderate intrauterine growth restriction(IUGR). Apparently normal neurosonoanatomy with normal ventricular width was noticed. Normal Doppler flow parameters of fetal (umbilical artery, middle cerebral artery) and maternal side (uterine arteries) and moderate polyhydramnios were observed. Outstanding observation was the permanent immobility of the entire fetus in 4D-US. The fetus was in breech position with extended legs, the tongue was protruding from a slightly gaping mouth with moderate retrognathia, and the fists were clenched. We found during our two US examinations an abnormal KANET test, the first at 30w2d with a score of 3 points, and the second at 31w4d, with a score of 4 points. Cardiotocography (CTG) demonstrated complete loss of variability and accelerations, in repeated CTG samples with registration over more than 30 minutes each. (Fig.1)
We discussed the abnormal findings with the parents and suggested amniocentesis for kariotyping which was carried out at 30w3d. The cytogenetic report confirmed 46,XX without numerical and structural chromosomal anomalies. Parvovirus-PCR in amniotic fluid was negative. Acetylcholinesterases and alpha-fetoprotein levels in amniotic fluid were normal. At 32 weeks, our patient decided to travel to USA for delivery. There she developed at 33 weeks severe polyhydramnios with breathing difficulties, back pain and sleep disorder. At 34 weeks, 3,5 liters of amniotic fluid were drained for amniocentesis. The procedure was followed by onset of labor. The preterm female baby was born at 34w2d through low transverse C-section because of breech position. The baby was delivered without cries or respiration and successfully intubated on third attempt at 17 minutes post delivery and continued on positive pressure ventilation. The clinical manifestation of severe contractures, the Pena-Shokeir phenotype and the akinesia indicated the possibility of neurologic disturbance, as described below in the neuropathology report. The possibility of an intrauterine insult was considered more likely than a genetic syndrome. Postnatal brain MRI showed global volume loss of hemispheres and cerebellum, EEG diffuse low voltage and slow activity consistent with severe encephalopathy, and US demonstrated findings of bilateral intraventricular hemorrhage and increased echogenicity of bilateral basal ganglia. After extensive discussion of the catastrophic brain damage with the parents, the baby was compassionately extubated on day 5 post partum and passed away 30 minutes after extubation. The parents requested autopsy. In the process of retrospective case evaluation, we experienced the mother as full of trust and very cooperative. She was able to speak about ‘the baby which had stopped moving’. Appropriate counseling and mental preparation of the parents for an unfavorable pregnancy outcome was based on four dimensional ultrasound (4D) evaluations of the fetus, showing repeated abnormal KANET an revealing the true extent of fetal compromise by means of understandable 4D video sequences. After seven months the patient was pregnant again and came for ultrasounds 2nd trimester scan. (10)
Absence of the mother during pregnancy, with its implications for different forms of maternal communication with the fetus like speaking, singing, touching and holding of the womb, can be seen in illicit drug abuse. Substance use severely reduces a woman’s ability of transition into the emotional achievements of motherhood, a task vital for a successful bonding process and loving relationship with the fetus. (11)
Working in Hosting Centers for women and children, we have gathered a great experience of cases with problems in mother/child relation, since pregnancy.
We are reporting a case of an 18 years old mum of 2 babies. The elder was 1 and half year and the youngest 2 months.
The girl, that we are going to call Maria, had a violent relation with her husband. The family was well-known by the Social Services since 2 generations. They were considered “nomads” because they did not have their own house and kept moving from one parents’ house to the other’s. This is a recurring characteristic of Maria’s family since her mother, who was 16 when she got pregnant, had spent some years with Maria’s father, a tumbler who moved for working reasons. When Maria’s parents divorced, the baby was greeted with her mother by a foster family. Few years later her mother married again and was able to provide for her daughter’s needs.
Investigation has revealed that there is a recurring trauma in previous generations: the destiny of abandoned child. Maria’s mother was left by her mother at the hospital and grown up by her fathers’grandparents.
The Hosting Centre staff in charge for the observation of mother/child relationship, reported that Maria did not want her second baby. She was leaving the newborn alone crying in the bedroom and did not care of her. She did not want to feed the baby and did it only at her left breast while with the right hand was chatting with her husband.
It was a typical case of puerperal (postpartum) psychosis, according to H. Ey definition. S.Fanti has called it “false-presence mother”: a new mother unable to take care of the newborn, that she feels as an unbearable burden. Maria considered herself incapable to be a good mother and had a cold interaction with her elder child too. The 1 and half year baby had a depressive mood, he was non interested in surrounding ambience, he didn’t look for interaction neither with her mother, nor with other people or children.
Two months later the observation was interrupted, because Maria left her children at the Hosting Centre and reached her husband. The staff referred that separation occurred without any particular emotional stress.
“The family is a vocation” N. Peluffo said ” even though it seems to be a necessity. Reproduction instinct is definitely a biological necessity, which does not involve automatically the constitution of a family. Anomaly in reproduction instinct is a pathological evidence related to death drive”.
By mentioning the word “vocation”, Peluffo did not mean that somebody is calling you to accomplish a certain job. In order to grow up and protect children for the time they need it, that for human being is much longer than for other races, parents should be able to identify themselves to the good-caring image of parents and establish emotional bond with their children. If these characteristics are missing, procreation is just the biological need to fulfill emptiness feeling caused by lack of object relation (parental bonding).
Lack of object relation is experienced in different ways:
1. endless feeling of inadequacy and deficiency
2. incapability of being independent.
These people usually have ambivalent relationship with anyone and anything, including parts of themselves or their body. They are inconstant in each activity. They can get very excited at the beginning, but then they loose interest, as soon as the object does not correspond to their expectations. Moreover they are always depending on something or somebody, usually a partner mostly similar to them.
In private practice with long sessions of intensive psychoanalysis, we have collected many cases that can demonstrate such affections.
We are reporting the case of a young lady, married to a 20 years older man, who was suffering anxiety neurosis, (according to Freud’s classification of psychopathological disorders. Nowadays is commonly used “panic attack” definition).
She was referring neurovegetative symptoms and agoraphobia, which appeared each time she had lost a beloved person, object or wellknown situation. The object had represented for a certain time her ideal object and she left it when she became disappointed.
She was an only child, abandoned in early age by her parents and grown up by the grandmother, that for many years was the only person on whom she could count on. Unluckily the grandmother had suffered the same trauma in childhood and had developed a dependent personality disorder.
For several years the young lady had been looking for a baby, but she couldn’t get pregnant. She was ambivalent toward pregnancy, she had achieved a good financial position which permitted independence from her husband. The grandmother had passed away and she could finally enjoy some freedom, but nevertheless, compulsion to repeat was unconsciously driving the patient to return to a dependent situation. She was pretty sure that a big family with many children was the only escape from loneliness and also the way to avoid the destiny that afflicted the women of her family who had lost their husbands in wars, road accidents or suicide.
During pregnancy a woman experiences again her own gestation and symbiotic intrauterine relation is repeated. Regardless of the fetus sex, pregnancy represents the essay to repair our and our mother’s castration fantom, but birth unavoidably repeats lost/castration feelings.
“When a woman delivers her baby, who is the phallic representative of her completeness” says Peluffo, “the baby, at the same time looses the placental symbiosis with the mother and has his first unchangeable experience of loss…Since placenta is an organ belonging both to the mother and the fetus, it represents their conjunction”.(Nathanieltz, 1987) “Placental castration is necessary for mother and child survival and is also the prototype of following stages’ castration”. (12)
Psychic traces of such loss experience, motivate the continuos search for a “place”. In other words it motivates the search for a relation, where we can find our psychobiological completeness.
Psychoanalytical relation is one of the displacement in this endless search.
The patient finally got pregnant at 45 years and right after first ultrasounds screening she got disappointed because the baby was a female. She tried to deny her disappointment and castration feelings during pregnancy through investment on the self, more precisely, on a narcissistic image of herself completed and not castrated. The birth confirmed the castration and consequently the patient experienced also an unconscious reject of the baby. She couldn’t feed the newborn and take care of her. She protected the child against her disappointment (a manifestation of aggressiveness), going back to work one week after delivery and left the little girl with a nurse. The baby grew up healthy, but of course nurse was the only person she was attached to. At eight months she did not recognize the mother yet, she was not looking for interaction with her, did not cry when she was leaving and later on she even refused food when her mother tried to feed her. At three years she looked as a little,old, sad lady without any vital light in her eyes. Educators of the kid-garden said that the little girl did not play with other children and was not interested in exploring the environment.
It is worthwhile to analyze the neurovegetative symptoms of the patient. According to Freud, they are connected to sexual abstinence or unsatisfaction.
Nevertheless we should remember that symptom is overdetermined, as any other unconscious manifestation and it can realize several desires at the same time, for example the realization of incestuous child desire (according to the infantile fantasy that mum gets pregnant by eating and abortion occurs by throwing up).
Symptom is connected also to the ambivalence expressed by the detain/expel dynamic in relation to the symbiotic object. It realizes at the same time the regression desire to embody a pre-adolescent image which denies castration. A jung prepubertal girl or boy is not sexually determined yet and can unconsciously wish to become an hybrid with both female and male sexual attributes. A complete sexual development definitely states sexual identity and forces the female to accept her castration. Sexual development states as well sex complementarity and that the only way to repair fantasmatic castration is sexual reproduction.
Whenever this narcissistic wound is not overcome through sexual reproduction, the subject tries different ways: repeating search for the right partner, pregnancies, jobs and also through psychoanalysis, but nothing is satisfactory, a part from rare moments during pregnancies. Disease and symptom seems to be the easiest solution, certainly the most economic and in case of neurovegetatitve and eating disorder symptoms, they provoke regression to precocious stages of development.
In Three essays on the theory of sexuality Freud says: ” the symptoms are the converted expression drives that would be defined as perverse if they could express themselves directly, without deviation of consciousness, in resolutions of fantasy and actions….neurosis, let’s say, is the negative of perversion.”(13)
Conclusions
4D or real time 3D permits to see the fetal life and recognize the fetus as an independent human being. Without any doubt it’s a great instrument to early development of mother-fetus relation.
Nevertheless, in those people characterized by strong narcissistic nucleus, psychic defenses such as isolation and splitting, can be so hard to make the subject waterproof even to the images of his child in the womb.
Nevertheless we hope that a tight cooperation between gynecologists and psychotherapist, will lead to new discoveries and open the way for integrated treatments.
Dr Ulrich Honemeyer – Dubai Emirates
Dr Bruna Marzi – Bergamo Italy ©
Notes:
1. Mellor DJ, Diesch TJ, Gunn AJ, Bennet L. Fetal ‘awareness’ and ‘pain’: What precautions should be taken to safeguard fetal welfare during experiments? AATEX 14, Special Issue, 79-83 Proc. 6th World Congress on Alternatives & Animal Use in the Life Sciences August 21-25, 2007, Tokyo, Japan
2. Lecanuet J P, Schaal B.Sensory performances in the human foetus: a brief summary of research. Intellectica, 2002/1, 34, pp. 29-56
3. (Schaal B, Marlier L, Saussignan R. Human foetuses learn from their pregnant mothers diet. Chem.Senses 25:729-737, 2000)
4. Smotherman WP, Robinson SR. Odour aversion learning by the rat fetus.Physiol.Behav.,29, 769-771
Bilko A, Altbaecker V, Hudson R.(1994) Transmission of food preference in the rabbit: the means of information transfer.Physiol.Behav.,56, 907-912
5. Kirstein CL, Philpot RM, Dark T. (1997) Fetal alcohol syndrome: early olfactory learning as a model system to study neurobehavioral deficits. Int. J. Neurosci., 59, 119-132
Kandel DB, Wu P, Daies M.(1994) Maternal smoking during pregnancy and smoking by adolescent daughters. Am J. Publ. HIth, 84, 1407-1413
6. Moore JK, Linthicum FH. The human auditory system: A timeline of development. 2007, Vol. 46, No. 9 , Pages 460-478
Graven S N, Browne J V. Auditory Development in the Fetus and Infant 2008 Published by Elsevier Inc.1527-3369/08/0804-0278
7. Lecanuet J-P, Granier-Deferre C, Jacquet AY, Capponi I, Ledru L. Prenatal discrimination of a male and female voice uttering the same sentence. Early Development and Parenting 1993; 2: 217-28.
8. Visual evoked responses were measured in fetuses from 28 weeks’ gestation onwards.
Magnetoencephalographic recordings of visual evoked brain activity in the human fetus. The Lancet Vol. 360, Issue 9335, 7 September 2002, Pages 779–780
9. Castiello U, Becchio C, Zoia S, Nelini C, Sartori L, et al. (2010) Wired to Be Social: The Ontogeny of Human Interaction. PLoS ONE 5(10): e13199. doi:10.1371/journal.pone.0013199
10. S. Fanti: Dizionario di psicoanalisi e micropsicoanalisi, Borla, Roma 1984
11. G. Ternavasio: Interista a Nicola Peluffo, www.psicoanalisi.it
12. N. Pelulffo: La relazione psicobiologica madre-feto, Borla, Roma 2010
13. S. Freud: Tre Saggi sulla Sessualità: ed Boringhieri
EDUCATION:
June 1970 High School Diploma Schloss-Gymnasium Benrath, Duesseldorf, Germany
1970 to 1971 Medical studies in Liege, Belgium
1971 to 1977 Medical studies in Goettingen ,LeibnitzUniversitaet,
and Berlin,FreieUniversitaet Berlin
January 1977 Exam of the American Educational Commission for Foreign Medical Graduates
ECFMG, Berlin
February 1977 German Medical State Examination with overall score: very good
March31, 1978“Approbation alsArzt”(License to practice medicine)
1980, June Research doctorate “cum laude”,FreieUniversitaet Berlin
Thesis in Angiology/Radiology
“ DieTranslumbaleAortographie-Wert der translumbalenAortographiealsAlternativ-TechnikzurtransfemoralenSeldinger-Technik “
POSTDOCTORAL TRAINING:
1977 to 1978 InternshipDept.of Internal Medicine ,and Dept.of Surgery Martin-Luther-Hospital
Grunewald,Berlin
1978 to 1980 ResidencyDept.of Radiology and Radiotherapy, Martin-Luther-Hospital,
Grunewald, Berlin.
1980 to 1981 ResidencyDept.ofSurgey,Martin-Luther-Hospital, Grunewald, Berlin.
1981 to 1983 Residency Dept.of Obstetrics and Gynaecology,WaldkrankenhausSpandau,Berlin
1983 to 1987 ResidencyDept.of Obstetrics and Gynaecology, KreiskrankenhausSigmaringen,
Teaching Hospital of University of Tuebingen/Baden-Wuerttemberg
1987 to 1989 ResidencyDept.of Internal Medicine,Pfullendorf,Baden-Wuerttemberg
1990 to 1991 ResidencyDept.of Obstetrics and Gynaecology, University of Essen
OTHER POSITIONS:
1989 to 1990 General Practitioner (GP) in Flying Swiss Ambulance Rescue Service(FSAM)
In Male, Maldives
1991 to 2003 Consultant Ob/Gyne ,Nabburg Hospital, Oberpfalz,Bavaria
2003 to present Consultant Ob/Gyne,Welcare Hospital EHL, Dubai
MEMBERSHIPS IN PROFESSIONAL AND SCIENTIFIC SOCIETIES:
-Deutsche GesellschaftfuerGynaekologie und Geburtshilfe 1997-2003
-BayerischeGesellschaftfuerGeburtshilfe und Frauenheilkunde 1996-2003
-GesellschaftzurFoerderungeinernaturwissentschaftlich-physiologisch
begruendetenAkupunktur ( NPA ) 1999-2003
-German Society of Anti-Aging Medicine( GSAAM ) 2001-2003
-International Society of Ultrasound in Obstetrics and Gynaecology 2005-present
LEADERSHIP POSITIONS IN PROFESSIONAL & SCIENTIFIC SOCIETIES:
2010 to present Co-director Ian Donald Schoolfor Medical Ultrasound,Dubai
2010 to present Executive director of Advanced Course Ultrasound Ob/Gyne Ian Donald
School, Dubai
TEACHING ACTIVITIES:
2010 February Appointment by Ian Donald School Headquarters as teacher for hands-on
training of postgraduate students for Fellowship of Advanced Ultrasound in Obstetrics and Gynecology















{kind=link}